Happy Childhood Village
AN INTRODUCTION To Happy Childhood Village, kISONGO, Tanzania, In Progress
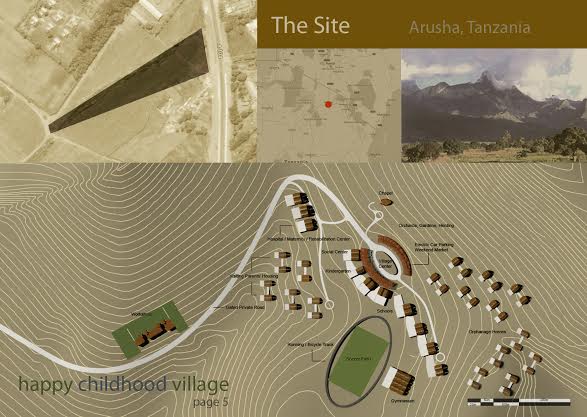 |
Site Map, Happy Childhood Village, Arusha, Tanzania, Debbas Architecture, In Progress
|
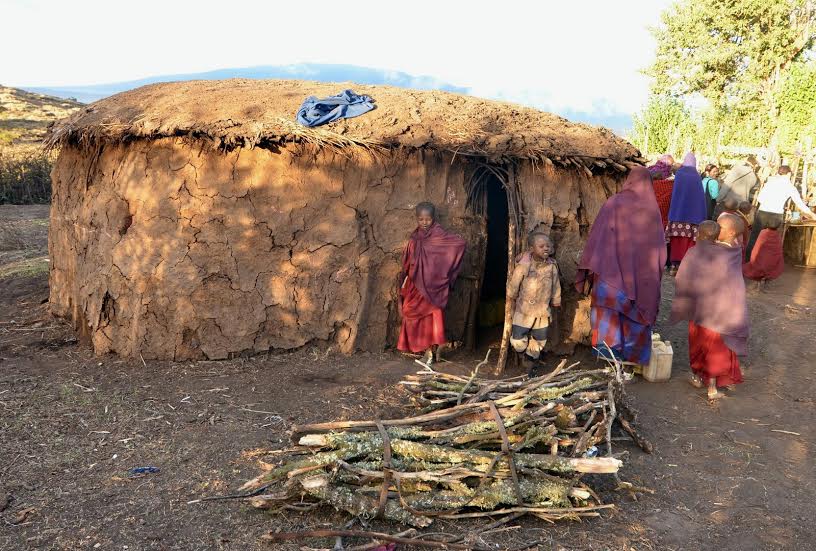
The Happy Childhood Village is a concept for a grounds-up community that will cater to local orphans (many with AIDS) as well as children whose parents are unable to care for them. Debbas Architecture, a firm based in Berkeley, California that is led by Charles Debbas. In addition to homes, the firm is also building a school for 450 children, a pre-school and day care center, a social center, a rehabilitation center (for children with disabilities), a maternity ward, homes for visiting parents, a gymnasium and soccer field, 10 workshops, a plaza for festivals, open markets, as well as a chapel.
It is not replacing any existing villages nor is it displacing anyone. The Happy Childhood Village will be located in Kisongo near the City of Arusha. The site faces Kilimanjaro, is relatively green with rolling hills.
The project is being funded by private donors and was initiated by an individual as a way to honor the memory of the son he lost. The land is being donated by the archdiocese of Tanzania. The architects are working pro bono. The project has grown in size and scope tremendously since the initial concept and is becoming, even at this stage, the template for other similar projects worldwide.
For those interested in how a project such as this is accomplished, the following is a concept document that lays out many of the details.
Concept Document
Background Research
- Size and scale of the problem
- 23.5 million people with HIV / AIDS live in Sub-Saharan Africa (UNAIDS, 2012).
- 15.3 million orphans < 15 years old.
- In Tanzania: 3 million orphans; 1.3 million of whom orphaned by AIDS; only 30% receive some sort of support. Support is concentrated mostly in urban centers.
- Population of Tanzania = 47.78 million. 44.8% below 14 years old. Life expectancy 60.85 years.
- National prevalence of HIV in Tanzania 6.2%; with some parts of the country recording 32% HIV occurrence among pregnant women.
- The biggest impact of HIV/AIDS pandemic is the orphaning of children below 15 years old
- Children below 15 years of age account for 1 of 6 AIDS-related deaths worldwide and 1 of 7 new HIV infections, mainly through mother-to-child transmission of the HIV virus.
- Impact on overall community:
- Decline of life expectancy and median age -> dependent portion of population increase as # of orphans increase relative to dying adults
- High mortality rates among adults due to HIV / AIDS has contributed to weakening of the extended family system
- Biological and extended family disintegrate because of HIV
- Orphans became victims of psychosocial and emotional problem
- The number of orphans in Sub-Saharan Africa is growing and number of caregiver is shrinking. Fostering worsens poverty situation of no-income / low-income families, increases marginalization and worsen their health and nutrition (UNICEF, 2006).
- AIDS and the resulting orphanhood thus has a profound impact on family systems and the community at large.
- Affected children are in danger of falling into poverty, stigmatization, discrimination, sexual abuse, migration and homelessness. They are liable to:
- Forego schooling
- Become married or pregnant
- Experience child labor
- HIV infection
- Other vulnerabilities
Note:
-Malaria, not HIV/AIDS, is the #1 cause of orphanhood.
-Number of orphans in Asia = 71.3 million > than Africa 53.6 million.
Defining vulnerable children
- UNICEF and global partners define an orphan as a child who has lost one or both parents.
- This definition contrasts with concepts of orphan in many industrialized countries, where a child must have lost both parents to qualify as an orphan. UNICEF and numerous international organizations adopted the broader definition of orphan in the mid-1990s as the AIDS pandemic began leading to the death of millions of parents worldwide, leaving an ever increasing number of children growing up without one or more parents. So the terminology of a ‘single orphan’ – the loss of one parent – and a ‘double orphan’ – the loss of both parents – was born to convey this growing crisis.
- However, orphanhood is not an event at a single point in life time, but rather a transitory phase. Orphanhood is experienced more as a gradual process than a single event. Children become orphans and disadvantaged long before their parents die because of the "time lag" between infraction and death which reduces adult capacity to be productive and provide resources for the well-being of their children.
- Most orphans assisted and cared for their dying parents. This is a significant constraint on the quality of their childhood
- It is important to realize that orphanhood is not the only cause of vulnerability. Poverty and household location are rather more significant causes of vulnerability. At the same time, being an orphan doesn't necessarily lead to vulnerability. Thus the need for a broader definition of targeted children.
Note:
In this document we will use the term Most Vulnerable Children (MVC) to refer to children, orphans or not, who are subject to vulnerability that impedes their development
- In general, vulnerable children may be:
- Living in poverty
- HIV-infected
- Without adequate adult support at home
- Experiencing chronic illness or disability
- Residing in poor living environment
- Experiencing inadequate access to education, health and social services
- Marginalized
- Stigmatized
- Discriminated against
- MVCs is a growing population with multi-dimensional needs
- Addressing their needed is a priority for donors, NGO's, and governments. This is not a policy issue, but requires effective programming.
What are their needs
- Majority of orphans have extremely poor living conditions and can not afford basic items such as food and clothing.
- MVC's have multifaceted needs, which include:
- Physical needs (e.g., food)
- Material needs (e.g., clothing)
- Intellectual needs
- Psychological needs
- Safety needs
- Physical and material needs are the most visible. The other needs are less visible to care providers.
- The children don't understand the situation of their parents death. They can't express their feelings and have no one to listen to their concerns.
- Children need to be loved, respected and listened to for them to be able to develop a health mind (UNAIDS, 2001)
- Psychosocial needs are fundamental to MVC care. Good mental health for children and adolescents is a prerequisite for optimal psychological development, productive social relations, effective learning and ability to care for oneself physical health and effective economic participation (World Health Organization).
- Policy formulation rarely address the needs of the plight of these orphans (UNICEF, 2003)
- International community and local governments have been slow to respond (UNICEF)
- Understanding the 8 Functions of family systems help identify the dimensions of intervention required to foster MVC's. These functions are:
- Affection
- Self-esteem
- Spiritual
- Economics
- Daily care
- Socialization
- Recreation
- Education
- Parents particularly play an important role to support intellectual, emotional and self-esteem needs of their young children.
- Therefore, when the direct family system disintegrates, children are hurt by lack of support on all of the above dimensions.
- After losing their parents, children may become emotionally unstable.
- Feeling of hopelessness, unhappiness and frustration are among the most prevailing feelings in MVC's. What bothers children most about the loss of their parents is the loss of emotional support (love and care).
- Stigma is another major hurdle faced by MVC's. They are often discriminated against, which further increase emotional distress.
- MVC's thus have exceptional educational needs because they suffer anxiety, grief, trauma, depression, stigma, and discrimination. Therefore, typical education (national curriculum) does not address there needs adequately.
- Gender and age influence the type of care expected and duties carried by children.
- Rural vs. urban divide in the ability of families to provide care.
 |
Rendering, Happy Childhood Village, Debbas Architecture, In Progress
|
Available care/ fostering options
- When parents die of HIV, several levels of care (safety nets) may be available for the orphan
- A child-headed or youth-headed family (siblings; older takes care of younger)
- Grandparent-headed family (usually, maternal grandmother if alive and has the capacity)
- Extended family (aunts and uncles)
- Community-based care (through volunteers)
- Foreign-sponsored Institutional care (e.g., orphan villages)
- Children who slip through this system of care, ends up as street children subject to exploitation, child labor, and prostitution, etc.
- Grandmothers take on caring of their orphan children under informal arrangements with minimal support from extended family, community, and the state.
- The role of the extended family is debatable. The extended family seems on the verge of collapse in some areas in Tanzania due to poverty, migration and the rise of capitalist value systems.
- The quality of care provided by the extended family is most often dependent on the state of relationship between the adopting family and the diseased parent.
- As the extended family mobilizes and modernizes, individualism increases and the family fragments. As a result, young MVC's are more likely to be alone in facing the psychosocial and emotional challenges. They experience:
- Extreme poverty
- Migration frustration
- Social stigma
- Breaking of kin ties
- Weak community support
- Lack of policy commitment by governments or foreign donors
- Lack of access to retroviral drugs
- Limited access to schools and deteriorating school performance
- Low self-esteem
- Depression
- Isolation
- Insecurity
- MVC's drop out of school as their parents become extremely ill and need care.
- Poverty complicated the situation of these children, for example although schooling is free, charges for uniforms, books, etc. can be prohibitive for the poor.
- Orphan villages tend to discriminate, stigmatize, encourage a sense of victimhood in the orphans, as such they were disempowering and instilling a sense of entitlement and privilege to MVC's over and above other non-orphan children.
- Focus on victimhood without fostering any asymmetrical reciprocity is counter productive
- Orphan children are not passive recipients of care. They have capacities that can be enforced to foster their well-being and development. They can potentially transform into agents for development for themselves, their direct and extended family, and their community. As such, the view of orphans as "burdens" is limited, discriminating and defeating.
- The one dimensional view of orphans as "burdens" not only overshadows the meaningful contributions they make to their families, but also diverts attention away from interventions grounded in their felt needs and capacities.
- The role of orphans in household livelihood is central and dynamic, governed by verying forms of reciprocity and care in which the flow of resources—material, social and emotional—are embedded in mutual expectations and support.
- Community care of the MVC has a crucial role of empowering them to take an active role in building their self-esteem and resilience, which make them achieve.
- According to the UNICEF (2004), even cultures and communities with strong social cohesion and traditions of providing support to orphans and MVC's can be overwhelmed when rate of increase and overall number of orphans reach high levels.
- All these social safety nets are overwhelmed and need restructuring and moral support.
- Community-based care of MVC has been recommended thus far as a cost-effective and culturally-fit care in Sub Saharan Africa; however, community-based care remains erratic, its quality of community-based care, which is delivered through assigned or elected volunteers is neither measured nor monitored.
State of existing services / programming
- Attention to MVC needs hasn't been adequate (UNICEF, 2012).
- Large scale programmes have included services in health, social support, economic strengthening, education, shelter, food security & nutrition and child protection.
- Sustainable interventions that leads to a long-term improvement in children well-being is a challenge.
- Human development is shaped by the outcome of interaction of the individuals with their environment.
- 4 layers (micro, meso, exo, and macro) must be considered when designing interventions with the child at the center. The child's development is determined by the settings (home, school, play, etc.) in which they spend time and the interaction with the members of these settings (care providers, teachers, peers, etc.).
- Programs targeting one layer (e.g., micro) will not produce quality impact as programs that target and engage multiple layers at the same time.
- Single-sector focus (e.g., only education or only health) has lead to suboptimal effectiveness and poor sustainability.
- Multi-sectoral programming not only reinforces development outcomes for children, families and communities, but also ensures long-lasting and sustainable outcomes.
- Regular schools are not meetings the educational needs of MVC's. A special curriculum that caters for emotional, physical, social, and spiritual needs is required.
- There is an evident lack of formal counseling services (due in part to cultural impediments).
 |
Rendering, Happy Childhood Village, Debbas Architecture, In Progress
|
Lessons learned
- Organizing at the local village is a must: build on existing local skills and available capacity and introduce "external" skills to advance capacities and motivate (local partner + knowledge / expertise partner).
- Projects must have tangible and measurable achievements. Unless improvement in local's well-being is sensed, locals won't persist on participating and contributing to the project.
- Local organization must be linked with existing infrastructure support (e.g., credit markets, government programs, local partner resources) and contributing to local economy.
- Reliable and sustainable source of funds from multiple sources.
- Must recognize the possibility of natural or man-made disaster.
- Sustainability
- Involvement of partners and donors [technical partners and donors must be distinct groups to avoid conflict of interest]
- Selective sustainability of key projects
- Sustainability has front-loaded costs
- Long-term view + flexible partnerships is key
Summary of key takeaways
- Children vulnerability is a significant problem of a growing magnitude
- Sources of vulnerability of children include but are not limited to orphanhood, which should be viewed as a transitory phase of the child's development (or lack thereof), beginning with the child's parent(s) sickness.
- The increasing number of vulnerable children overwhelms the direct family, the extended family, as well as even the most socially cohesive communities.
- The needs of MVC's are multifaceted (scope) and multidimensional (scale). Addressing these needs effectively goes beyond policies to effective programming that enables service reach and richness (quality) and sustainability.
- Most large scale programs have focused on children's physical and material needs, which are usually the most visible needs of MVC's. Psycho-social and emotional support is rather lacking.
- Interventions should cater to emotional and psycho-social well-being of MVC's and should attend to differences in the needs of children based on gender and age.
- The landscape of available care to orphans and MVC can be categorized in 4 levels:
- Direct family (child- or youth- headed)
- Grandparent
- Extended family
- Community
- Foreign-sponsored institutions
- The first 3 levels of care are already stained, overwhelmed and in some instances disintegrating.
- Community-based care, which is usually volunteer-based, suffer from poor quality and measurable impact.
- Foreign-sponsored institutions are often challenged by sustainability and cultural issues.
- Children who fall through the cracks of these levels of care, due to their limited reach, capacity, etc., are destined to become street children subject to various forms of exploitation.
- It is important not to "victimize" MVC's or model them as passive recipients of services to which they are entitled. This narrow view of MVC's as "burdens" to the community is counterproductive. These children have capacities that can be built and enforced, so they become ambassadors of development in their community.
- These children have the right to develop into productive agents. At the same time, they have a responsibility towards their community to build their capabilities. Enforcing their human rights and building their capabilities go hand in hand in helping them overcome "unfreedoms" (poverty, illness, social isolation, emotional and mental stability, stigma, etc.) that obstructs their development and well-being. This requires multi-faceted interventions at the individual, family, and community level.
- It is true: "It takes a village to raise a child"
|
|
|
 Meeting Room, Amalgamated Dwellings, New York City, USASpringsteen and Goldhammer, 1929  Boundary Street Estate Workshops, London, UK, London County Council, 1899  Vending stalls, Hismen Hin-Nu Terrace, Oakland, CA, USA, Pyatok Architects, 1995  Workshops, Perseigne Housing Estate, Alençon, France, Lucien Kroll, 1979  BDD Chawls, Worli, India, Bombay Development Department, 1920  Campus for Magic Bus, Panvel, India, 2007, RMA Architects  Cantagallo, Peru  Casa do Ataide, Paraisopolos, Sao Paolo, Brazil, URBZ Brazil, 2013  Casa do Ataide, Paraisopolos, Sao Paolo, Brazil, URBZ Brazil, 2013  Casa Familiar, San Ysidro, Califonia, USA, Estudio Teddy Cruz, Ongoing  Community Toilets for SPARC, Mumbai, India, RMA Architects, Ongoing  The Construction of Low-cost Community Centres. New Delhi, 1978.  Dolma Ling Nunnery and Institute, Sidhpur, Dharmasala, India, MN Ashish Ganju, 1998 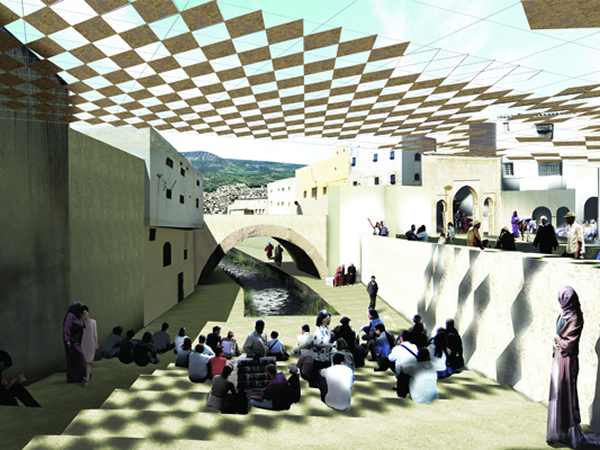 Fez River Project, City of Fez, Morocco, Aziza Chaouni Projects, 2012  Jungle Gym, Shivagi Nagar, India, Aditya Vipparthi and URBZ, 2014  KPSP, Kibera, Kenya, Koukuey Design Initiative, Ongoing  Lima, Peru  Livonia Commons, Brooklyn, NY, Urban Quotient, 2011  Manila, Philippines  Metrocables of Medillin, Medillin, Colombia, Edison Escobar and María Patricia Bustamante, 2004  Metrocables of Medillin, Medillin, Colombia, Edison Escobar and María Patricia Bustamante, 2004  Mother and Child Care Centre, Dakshin Habal Village / Bagman Village, West Bengal, New Delhi, MN Ashish Ganju, 1979.  Nairobi, Kenya  Solar Initiative, Various Locations, Mexico, BaSiC Initiative 2003-2010  Sudhir House, Saki Naka, Mumbai, India, URBZ, 2013  Technical Facilitation of Indira Awas Yojana In Gujarat, India, Hunnarshala Foundation, 2011  Bangkok, Thailand 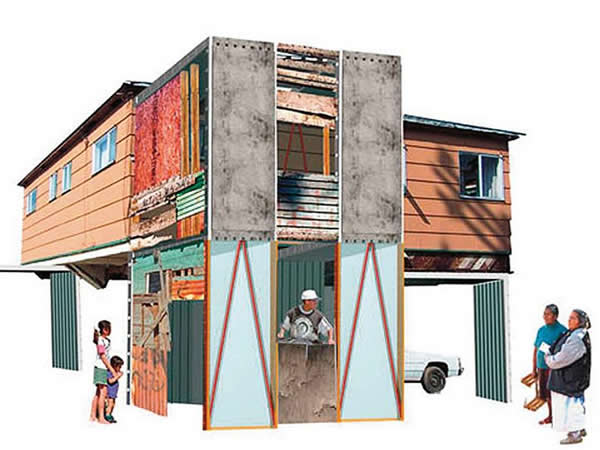 Manufactured Sites: Emergency Housing, Estudio Teddy Cruz  Low Cost Housing Programme, Karachi, Pakistan, Orangi Pilot Project, 1987  Floods: Relief And Rehabilitation, Sindh, Pakistan, Orangi Pilot Project, 2011  Dar es Salaam, Tanzania  Emma Cosio and her children are laying out the foundations of their house. Mexicali, Mexico, Christopher Alexander  Emma Cosio’s completed house in 1976. Mexicali, Mexico, Christopher Alexander 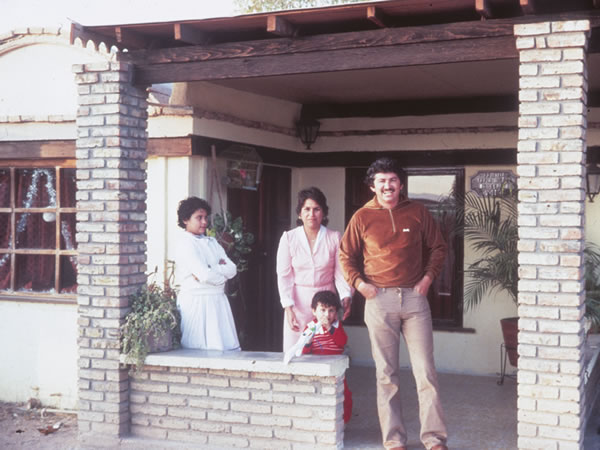 Jose Tapia’s house in 1976. Mexicali, Mexico, Christopher Alexander  Jose Tapia’s house in 1984. Mexicali, Mexico, Christopher Alexander 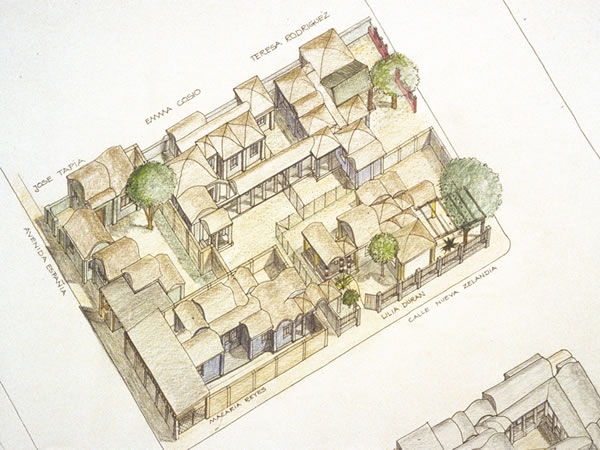 Mrs. Rodriguez in front of her home in 1984. Mexicali, Mexico, Christopher Alexander  The homes the five families built for themselves in 1976. Mexicali, Mexico, Christopher Alexander  Inside the Tapia’s home that they built with the help of students, 1976.  Tow Build - 1st workshop - Nansan Town Council Official brief 4th Architecture Students on the Planning & Housing challenges in Nabweru  Local market in the heart of Kampala  Local Resource and skills - use of sheet and timber to make house panel  View from Mutungo of the Ourskirts of Kampala  Participation - children sketching their dream house
|
|